

ACL Injuries and What You Need to Know
The anterior cruciate ligament (ACL) is one of the most physically, financially, and emotionally devastating sport related-related knee injuries.1 It can keep athletes from playing their sport that season and even end their career. The ACL is an important ligament in the knee because it prevents the tibia from moving forward and rotating. Since the knee has such a complex design it calls for a higher level of stability for regular function.2 When people think of knee injuries they often think of contact sports, but in fact, 70% of all ACL injuries are noncontact believe it or not.3 We have to ask ourselves why these types of injuries are occurring without contact with other players during sports and other athletic events.

All of the Forces That Can Act on the Knee
The knee has many different forces that act on it both biomechanically, muscles pulling on it, and the resistive forces from ligaments

Source: 24. Oh, Y. K., Lipps, D. B., Ashton-Miller, J. A., & Wojtys, E. M. (2012). What Strains the Anterior Cruciate Ligament During a Pivot Landing? The American Journal of Sports Medicine, 40(3), 574-583. doi:10.1177/0363546511432544
Usual Position of Non-contact ACL Injuries
- Rapid deceleration and change of direction, while foot is fixed, cutting or pivoting, plant maneuver, and/or one foot stopping or landing from a jump with knee in slight flexion or extension20-23
- Generally the tibia is rotated outward, knee is extended, femur is internally rotated and foot is planted.
Positions That Strain the ACL

- Internal tibial (sometimes external) torque combined with knee valgus24 aka knocked knees.
- Noncontact injuries occur when landing on a slightly flexed knee with internal tibial torque and contracted quadriceps to slow resist flexion24
- Lateral femoral condyle and posterolateral tibial plateau bone bruises are often found as well.25-27
- The slope of the lateral tibial plateau is a predictive factor28
- Inability to control tibia rotation during side stepping maneuvers23
How Much Force Does It Take to Tear an ACL?
The ACL is actually incredibly strong! The ACL has a tensile strength of 494.6 lbs.29,30 This means that you could hang 493lbs off of your ACL before it would tear! That is super strong! Without an ACL the tibia can translate forward with 30.1 lbs of force,31,32 making the knee more susceptible to injury. The quadriceps muscle alone can tear the ACL itself if it can generate 1,011.6 lbs of force with the knee at 20º of flexion.33
Healing Time Frames
Healing times can vary from person to person. Some factors that have been studied are age and the physical condition prior to intervention. The younger a person is the faster the recovery rate and the better physical condition a person is before surgery both lead to faster recovery times.
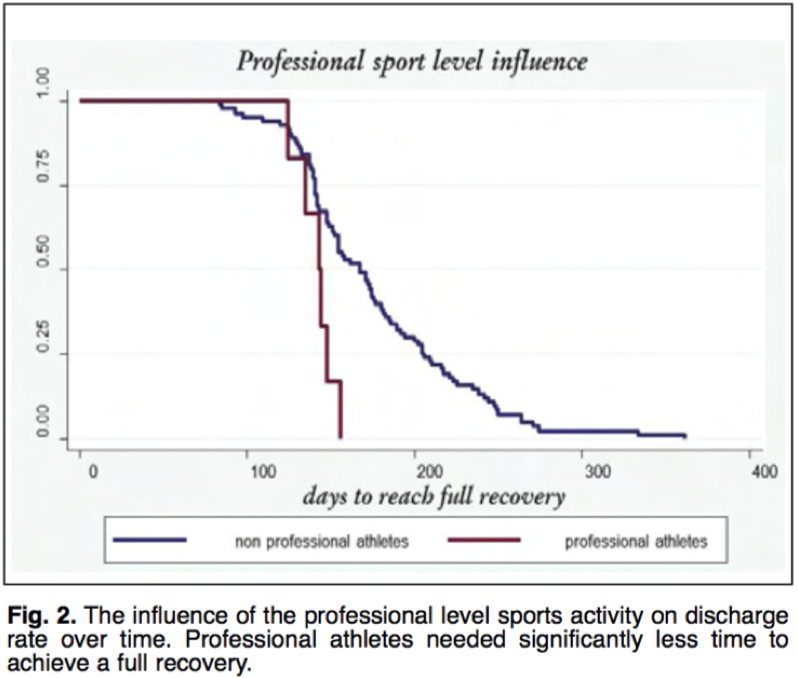
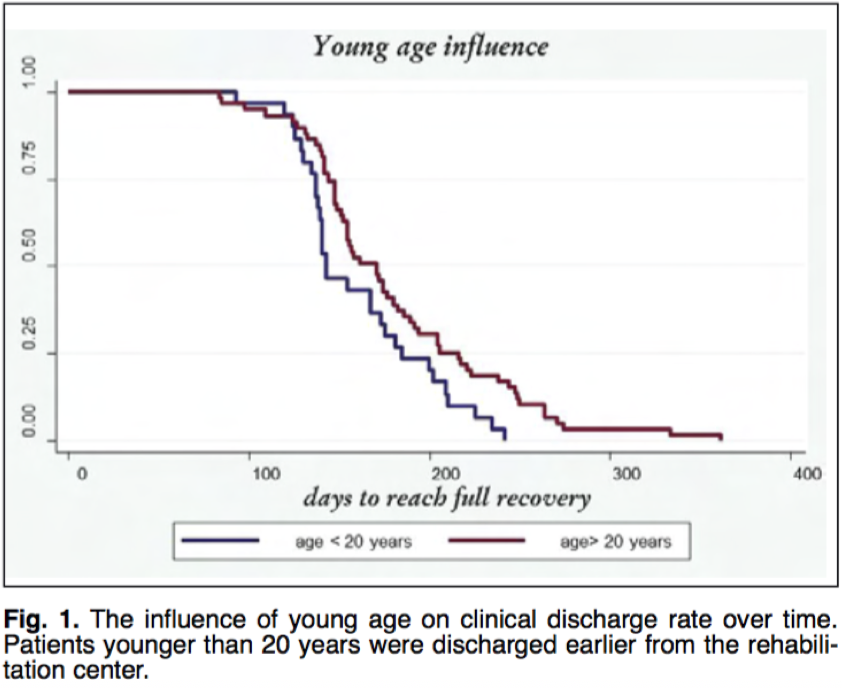
Resource: Villa, F. D. (2015). Anterior cruciate ligament reconstruction and rehabilitation: predictors of functional outcome. Joints. doi:10.11138/jts/2015.3.4.179
There are some researchers that say it surgery increases your risk of arthritis in the future depending on the amount of scar tissue that is left over and how invasive the surgery is. There is not enough evidence yet to support the statement that replacing the ACL will prevent osteoarthritiswith a slight increase from 37% to 44% if you get ACL replacement surgery.34 The biggest factor in osteoarthritis is a meniscectomy35 as well as obesity.
Strengthening Exercises Pre/Post Injury
•Closed chain exercises work best because they allow for compression of the joint which gives it more stability
- Hamstrings- should be 66%-75% strength of quadriceps21
- Quadriceps- maintain balance with hamstrings
- Hip abductors
- Hip external rotators
- Exercises that involve contracture of quadriceps and hamstrings together21
Rehabilitation

- Squatting 50-100 degrees of knee flexion puts the least amount of stress on the ACL36-45
- Forward and side lunge have minimal stress on ACL like a two legged squat.
- Leg press is a safe exercise
- Knee extension exercises should be done with resistance closer to the knee if performed46 to not add extra stress to the ACL and knee.
- Bracing after having surgery does not make much of a difference in most cases47
The Core and Its Role with the Knee
The core is often talked about a lot, but is often not described and varies who you talk to. For the purpose of this article I will refer to the core as the muscles of the hips, pelvis and lower back. Muscles included are;
- Latissimus Dorsi
- Pectoralis
- Transverse abdominals
- Quadriceps
- Hamstrings
- Iliopsoas
The purpose of the core is to provide stability for distal limb mobility. People who study the kinetic chain know that the core is involved in almost every movement of the body’s limbs .
2 Ways to Assess the Core
One-leg standing balance test
With a single leg standing test, when you lift one leg the hips should remain level, the body should be upright without arching the back or hunching forward.
One-legged squat
Performing a one legged squat can reveal many core imbalances as well as muscle coordination in and around the knee. When lowering the body, the supporting knee should not move towards midline. If this occurs your knee will be more prone to injury including your ACL.

The core allows for stability so the distal limbs can use it for an anchor to properly function7.
When the core is weak you will have a positive test like the pictures below. A weak core does not provide a good anchor for the leg.


Should I Stretch More?
Sometimes people think the solution to a lot of problems are to just stretch more. Stretching is only beneficial if your muscles and ligaments cannot move through their normal range of motion. Being too flexible can be just as detrimental as not being flexible. You want a good balance so work on whichever pertains to you and your body. If you have had an ACL replacement, stretching is critical during the rehabilitation process as the scar tissue is forming.

What Is Neuromuscular Control?

Neuromuscular control is often over looked when it comes to joint instability and dysfunction. The ligaments in your body hold the bones together, the muscles in your body move the bones and the nerves in your body tell which muscles to contract and when to contract. When the nerves fire correctly in a coordinated fashion then you have proper neuromuscular control.
- Neuromuscular training and re-education are important to rebuild the neurological pathways to muscles for coordinated movements.48
- Active stabilization of the knee is dependent on coordination and co-activation of the muscles around the knee49-51
- Neuromuscular control deficiencies are, at this time (2010), the only known modifiable factor predictive of second ACL injury risk52,53
- ACL injuries occur approximately 40 milliseconds after initial contact with the ground54
- Rehabilation should be geared towards limb symmetry and working on deficits55
- Cerebellum function is important for smooth continuous movements, timing of movements, error detection and correction while moving56-59
- People with cerebellar lesions often display deficits in movement velocity and acceleration making them more prone to injury60,61
- Neural fatigue can affect muscle function, making joints more prone to injury62
How to Increase Neuromuscular Performance of the Lower Body
- Getting adjusted and removing interference within the nervous system
- Plyometric workouts
- Single leg balancing
- Squatting
- Performing lifts with proper form
Does the Playing Surface Have a Role with ACL Injuries?

In the past all field sports used to be played on natural grass fields. With sports playing all year round turf fields have been introduced. The friction with the turf field is different than with grass fields. It has more cushion, meaning more give, and more potential for injury. During the NFL season 2002-2008 there was an 88% increase in ACL injuries when switching from grass to turf!!
What Else May Be Injured During an ACL Injury?
The cartilage in your knee is susceptible to injury during the time frame the ACL is torn and is more likely to get injured after the ACL is torn since the ligament is not able to keep the femur and tibia on track. The most common piece of cartilage that is prone to injury is the medial meniscus and the most common ligament is the medial cruciate ligament.
•Medial Cruciate Ligament (MCL) strain usually occurs 5lbs of force during knee abduction63 and 11lbs of force of internal tibial rotation63 This suggests the MCL strains would more likely to be secondary to ACL tears since ACL is under load where before MCL is.
The absence of a meniscus or a bucket handle tear with a torn ACL will have a higher impact on the kinematics more than just an ACL tear64
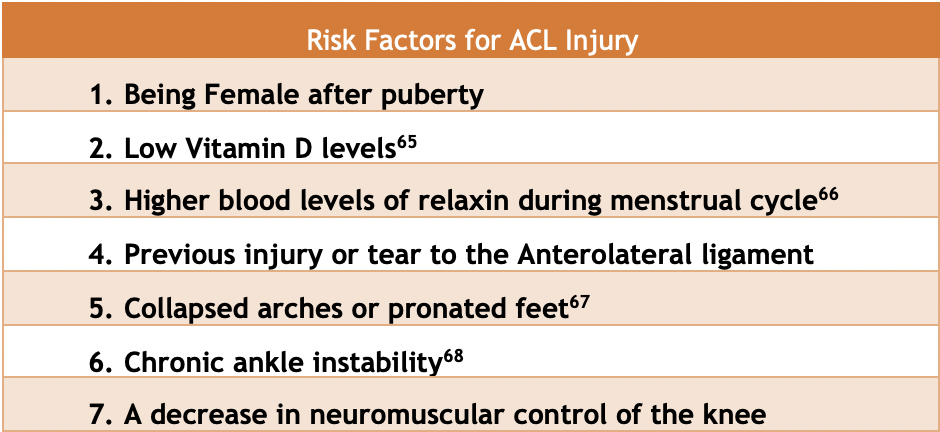
- Being Female
Being a female is a risk factor for a couple reasons. One reason is that they have wider hips generally increasing their Q Angle, stressing the ACL more. Their ligaments are not generally as strong overall compared to men, and their hormones can have an influence on the strength of the ligaments in the body.
- Low Vitamin D Levels
Vitamin D is good for reducing inflammation after surgery because inflammatory cytokines are increased during the post-surgical recovery time. Having normal levels of vitamin D concentrations >30ng/mL facilitates the healing processes and allow for better muscle contractions during the rehabilitation process. Low vitamin D levels are associated with muscular weakness.69
- High Levels of Relaxin Hormone
This hormone is released during pregnancy and make the ligaments in the female body more flexible and stretchable, preparing the body to expand the pelvis for the delivery of the baby.
- Previous Injury to the Anterolateral Ligament
This little ligament helps to prevent over rotation of the knee. If this ligament is injured, then the ACL will have to work harder to compensate for the lack of instability.
- Chronic Ankle Instability
Chronic ankle instability leads to fatigue faster allowing the knee to work harder and receive more forces that are normally handled by the ankle. Spraining your ankle over and over will make you more prone to injuring your ACL. If you keep spraining your ankle it is a good idea to get it checked out to see if it is in proper alignment.
- Decrease in Neuromuscular Control
The nervous system controls and coordinates all muscle movements within the body. If the nervous system cannot properly communicate with the muscles in a timely manner and in an organized fashion then functional instability will result in the joint making it more prone to injury.
How to Prevent ACL Injuries
- Strengthening exercises
- Maintain proper flexibility
- Improve neuromuscular control
- Work on skill set training to your particular sport
What Is Proprioception and How Does the ACL Affect It?
Proprioception is the term used to describe how the body and brain communicate. The body knows where it is in space from the signals being sent from receptors in joints, muscles and connective tissue. This is how we know where our body is in space with our eyes closed. All joints, muscles, ligaments and tendons give proprioceptive input into the brain letting the brain know where the body is in space.
- ACL deficient people have less proprioception and it actually changes some of a person’s neurology and diminishes activation in parts of the brain
- Anticipatory postural adaptations- create proximal stability for distal mobility72
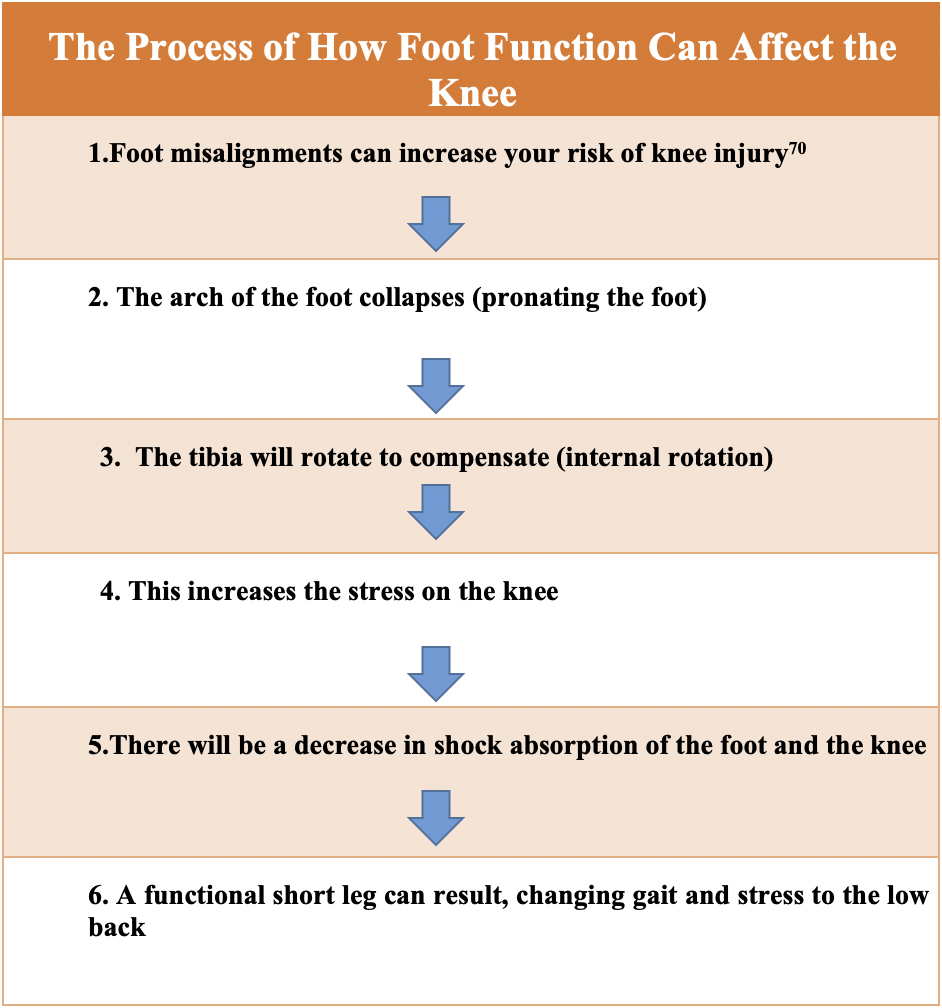
Foot function can affect the knee as well. It is important to have properly moving bones in your feet, good biomechanics of the ankle and good functional arches in your feet. Here is a diagram explaining how dysfunction in the foot can affect the knee as well as the rest of the body.
How Can Chiropractic Help?
Chiropractic works to align the spine and extremities so that the body moves better biomechanically while also removing nerve interference within the body. This improves muscle coordination and balances muscle tone between left and right side of the body.
- Adjustments can improve leg length inequality71 which can improve gait and limb symmetry, decreasing biomechanical stress on the body.
- Adjustments can change heel and foot pressure differences71 when comparing Left foot vs. Right foot
- Adjustments align the spine and lower extremity to make sure the biomechanics are fully functional.
- By aligning the pelvis we can change the mechanics and decrease the stress on the knee and foot that attach to the pelvis.
- We look to see how your body is functioning:
- Is your spine in alignment?
- Do you have nerve interference in your body affecting neuromuscular control?
- Does your spine move correctly? Proper motion of joints will help to prevent injuries in the future
How Do We Check to See if You Have Nerve Interference?
We use infrared thermography to measure the temperature of your back which is an indirect measurement of how balanced your nervous system is. If there are areas that are too hot or too cold, then it would indicate an imbalance within the nervous system since the nerves control the blood flow to your skin.
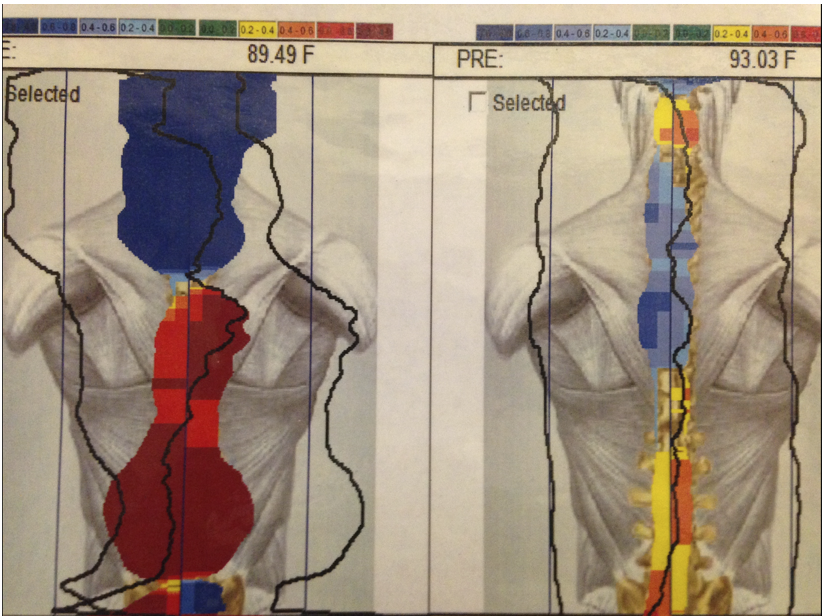
On the LEFT is someone who initially came into the office. On the RIGHT is the same patient after chiropractic care. The nerve interference has significantly reduced allowing the body to function better.
Resources for ACL Prevention Programs for Coaches
http://smsmf.org/smsf-programs/pep-program. Download PDF
www.Sportsmetrics.org – program and ACL certification program
https://www.luriechildrens.org/en-us/kohls-cares/sports/Pages/kipp.aspx
Resources:
- Stasi, S. D., Myer, G. D., & Hewett, T. E. (2013). Neuromuscular Training to Target Deficits Associated With Second Anterior Cruciate Ligament Injury. Journal of Orthopaedic & Sports Physical Therapy, 43(11). doi:10.2519/jospt.2013.4693
- Sinkjær, T., & Arendt-Nielsen, L. (1991). Knee stability and muscle coordination in patients with anterior cruciate ligament injuries: An electromyographic approach. Journal of Electromyography and Kinesiology, 1(3), 209-217. doi:10.1016/1050-6411(91)90036-5
- Mclean, S. G., Huang, X., Su, A., & Bogert, A. J. (2004). Sagittal plane biomechanics cannot injure the ACL during sidestep cutting. Clinical Biomechanics, 19(8), 828-838. doi:10.1016/j.clinbiomech.2004.06.006
- Ardern, C. L., Webster, K. E., Taylor, N. F., & Feller, J. A. (2011). Return to sport following anterior cruciate ligament reconstruction surgery: a systematic review and meta-analysis of the state of play. British Journal of Sports Medicine, 45(7), 596-606. doi:10.1136/bjsm.2010.076364
- Brophy, R. H., Schmitz, L., Wright, R. W., Dunn, W. R., Parker, R. D., Andrish, J. T., . . . Spindler, K. P. (2012). Return to Play and Future ACL Injury Risk After ACL Reconstruction in Soccer Athletes From the Multicenter Orthopaedic Outcomes Network (MOON) Group. The American Journal of Sports Medicine, 40(11), 2517-2522. doi:10.1177/0363546512459476
- Busfield, B., Kharrazi, F., Starkey, C., Lombardo, S. J., & Seegmiller, J. (2013). Performance outcomes of anterior cruciate ligament reconstruction in the National Basketball Association. Journal of Orthopaedic & Sports Physical Therapy, 43(11), 777-811.
- Lee, D., Karim, S., & Chang, C. (2013). Return to sports after anterior cruciate ligament reconstruction- a review of patients with minimum 5-year follow-up. Ann acad med singapore, 41, 385-395.
- McCullough, K., Phelps, K., & Spidler, K. (2012). Return to high school-and college-level football after anterior cruciate ligament reconstruction: a multi-center Orthopedic outcomes Network (MOON) cohort study. American Journal of Sports Medicine, 40, 2523-2529.
- Shelbourne, K. D., Sullivan, A. N., Bohard, K., Gray, T., & Urch, S. E. (2009). Return to Basketball and Soccer After Anterior Cruciate Ligament Reconstruction in Competitive School-Aged Athletes. Sports Health, 1(3), 236-241. doi:10.1177/1941738109334275
- Quatman, C. E., Quatman-Yates, C. C., & Hewett, T. E. (2010). A ‘Plane’ Explanation of Anterior Cruciate Ligament Injury Mechanisms. Sports Medicine,40(9), 729-746. doi:10.2165/11534950-000000000-00000
- Erpell, B. G., Scarvell, J. M., Ball, N. B., & Smith, P. N. (2012). Mechanisms and Risk Factors for Noncontact ACL Injury in Age Mature Athletes Who Engage in Field Or Court Sports. Journal of Strength and Conditioning Research,26(11), 3160-3176. doi:10.1519/jsc.0b013e318243fb5a
- Hultz, S. J. (2008). Mechanisms of Noncontact Anterior Cruciate Ligament Injury. Journal of Athletic Training,43(4), 396-408. doi:10.4085/1062-6050-43.4.396
- Voskanian, N. (2013). ACL Injury prevention in female athletes: review of the literature and practical considerations in implementing an ACL prevention program. Current Reviews in Musculoskeletal Medicine,6(2), 158-163. doi:10.1007/s12178-013-9158-y
- Arendt, E., & Dick, R. (1995). Knee Injury Patterns Among Men and Women in Collegiate Basketball and Soccer. The American Journal of Sports Medicine,23(6), 694-701. doi:10.1177/036354659502300611
- Berns, G. S., Hull, M. L., & Patterson, H. A. (1992). Strain in the anteromedial bundle of the anterior cruciate ligament under combination loading. Journal of Orthopaedic Research,10(2), 167-176. doi:10.1002/jor.1100100203
- Griffin, L. Y. (2006). Understanding and Preventing Noncontact Anterior Cruciate Ligament Injuries: A Review of the Hunt Valley II Meeting, January 2005. American Journal of Sports Medicine,34(9), 1512-1532. doi:10.1177/0363546506286866
- Morrey, B. (2010). Cost Analysis of Converting From Single-Bundle to Double-Bundle Anterior Cruciate Ligament Reconstruction. Yearbook of Orthopedics,2010, 163-164. doi:10.1016/s0276-1092(09)79629-4
- Zantop, T., Herbort, M., Raschke, M. J., Fu, F. H., & Petersen, W. (2006). The Role of the Anteromedial and Posterolateral Bundles of the Anterior Cruciate Ligament in Anterior Tibial Translation and Internal Rotation. The American Journal of Sports Medicine,35(2), 223-227. doi:10.1177/0363546506294571
- Miller, M. D., D. E. Cooper, and James J. Warner. “Sports Medicine and Arthroscopy Review.” Sports Medicine and Arthroscopy Review 3.4 (1995): 3-71. Web.
- Shimokochi, Y., & Shultz, S. J. (2008). Mechanisms of Noncontact Anterior Cruciate Ligament Injury. Journal of Athletic Training,43(4), 396-408. doi:10.4085/1062-6050-43.4.396
- Boden, B. P., Griffin, L. Y., & Garrett, W. E. (2000). Etiology and Prevention of Noncontact ACL Injury. The Physician and Sportsmedicine, 28(4), 53-60. doi:10.3810/psm.2000.04.841
- Shultz, S. J., & Schmitz, R. J. (2009). Effects of Transverse and Frontal Plane Knee Laxity on Hip and Knee Neuromechanics During Drop Landings. The American Journal of Sports Medicine, 37(9), 1821-1830. doi:10.1177/0363546509334225
- Cross, M. J., Gibbs, N. J., & Bryant, G. J. (1989). An analysis of the sidestep cutting maneuver. The American Journal of Sports Medicine, 17(3), 363-366. doi:10.1177/036354658901700309
- Oh, Y. K., Lipps, D. B., Ashton-Miller, J. A., & Wojtys, E. M. (2012). What Strains the Anterior Cruciate Ligament During a Pivot Landing? The American Journal of Sports Medicine, 40(3), 574-583. doi:10.1177/0363546511432544
- Graf, B. K., Cook, D. A., Smet, A. A., & Keene, J. S. (1993). “Bone bruises” on magnetic resonance imaging evaluation of anterior cruciate ligament injuries. The American Journal of Sports Medicine, 21(2), 220-223. doi:10.1177/036354659302100210
- Johnson, D., Urban, W., Caborn, D., Vanarthos, W., & Carlson, C. (1998). Articular cartilage changes seen with magnetic resonance imaging detected bone bruises associated with acute anterior cruciate ligament rupture. American Journal of Sports Medicine, 26, 409-414.
- Spindler, K. P., Schils, J. P., Bergfeld, J. A., Andrish, J. T., Weiker, G. G., Anderson, T. E., . . . Medendorp, S. V. (1993). Prospective study of osseous, articular, and meniscal lesions in recent anterior cruciate ligament tears by magnetic resonance imaging and arthroscopy. The American Journal of Sports Medicine, 21(4), 551-557. doi:10.1177/036354659302100412
- Lipps, D. B., Y. K. Oh, J. A. Ashton-Miller, and E. M. Wojtys. “Morphologic Characteristics Help Explain the Gender Difference in Peak Anterior Cruciate Ligament Strain During a Simulated Pivot Landing.” The American Journal of Sports Medicine 40.1 (2011): 32-40. Web.
- Miller MD, Cooper DE, Waerner JJP. Review of Sports medicine and arthroscopy. Philadelphia: WB Saunders; 1995. p.3-71
- Miller MD, Sports medicine. In:Miller MD, editor, Review of orthopaedics. 3rd. Philadelphia: WB Saunders; 2000. p. 195-200
- Zantop, T., Herbort, M., Raschke, M. J., Fu, F. H., & Petersen, W. (2006). The Role of the Anteromedial and Posterolateral Bundles of the Anterior Cruciate Ligament in Anterior Tibial Translation and Internal Rotation. The American Journal of Sports Medicine,35(2), 223-227. doi:10.1177/036354650629457
- Kondo, E., Merican, A. M., Yasuda, K., & Amis, A. A. (2014). Biomechanical Analysis of Knee Laxity With Isolated Anteromedial or Posterolateral Bundle–Deficient Anterior Cruciate Ligament. Arthroscopy: The Journal of Arthroscopic & Related Surgery,30(3), 335-343. doi:10.1016/j.arthro.2013.12.003
- Demorat, G., Weinhold, P., Blackburn, T., Chudik, S., & Garrett, W. (2004). Aggressive Quadriceps Loading Can Induce Noncontact Anterior Cruciate Ligament Injury. The American Journal of Sports Medicine, 32(2), 477-483. doi:10.1177/0363546503258928
- Lux, B., Gribble, P., & Pietrosimone, B. (2014). Osteoarthritis prevalence following anterior cruciate ligament reconstruction: A systematic review and numbers-needed-to-treat analysis. Journal of athletic training, 49(6), 806-819.
- Segawa, Hiroyuki, Go Omori, and Yoshio Koga. “Long-term results of non-operative treatment of anterior cruciate ligament injury.” The Knee 8.1 (2001): 5-11. Web.
- Boynton, Brian, G. Howe, R. Johnson, and B. Fleming. “The measurement of anterior cruciate ligament strain in-vivo.” Int orthop 16 (1992): 1-12. Web.
- Beynnon, B., and B. Fleming. “Anterior cruciate ligament strain in-vivo: a review of previous work.” Journal of biomechanics 31 (1998): 519-25. Web.
- Beynnon, B. D., R. J. Johnson, B. C. Fleming, C. J. Stankewich, P. A. Renstrom, and C. E. Nichols. “The Strain Behavior of the Anterior Cruciate Ligament During Squatting and Active Flexion-Extension: A Comparison of an Open and a Closed Kinetic Chain Exercise.” The American Journal of Sports Medicine 25.6 (1997): 823-29. Web.
- Escamilla, R. F., G. S. Fleisig, N. Zheng, S. W. Barrentine, K. E. Wilk, and J. R. Andrews. “Biomechanics Of The Knee During Closed Kinetic Chain And Open Kinetic Chain Exercises.” Medicine & Science in Sports & Exercise Supplement (1998): 48. Web.
- Escamilla, R. F., N. Zheng, G. S. Fleisig, J. E. Lander, S. W. Barrentine, G. R. Cutter, and J. R. Andrews. “The Effects Of Technique Variations On Knee Biomechanics During The Squat And Leg Press 887.” Medicine & Science in Sports & Exercise 29. Supplement (1997): 156. Web.
- Escamilla, Rafael F., Naiquan Zheng, Rodney Imamura, Toran D. Macleod, W. Brent Edwards, Alan Hreljac, Glenn S. Fleisig, Kevin E. Wilk, Claude T. Moorman, and James R. Andrews. “Cruciate Ligament Force during the Wall Squat and the One-Leg Squat.” Medicine & Science in Sports & Exercise 41.2 (2009): 408-17. Web.
- Escamilla, Rafael F., Naiquan Zheng, Toran D. Macleod, Rodney Imamura, W. Brent Edwards, Alan Hreljac, Glenn S. Fleisig, Kevin E. Wilk, Claude T. Moorman, Lonnie Paulos, and James R. Andrews. “Cruciate Ligament Forces between Short-Step and Long-Step Forward Lunge.” Medicine & Science in Sports & Exercise 42.10 (2010): 1932-942. Web.
- Escamilla, Rafael F., Naiquan Zheng, Toran D. Macleod, Rodney Imamura, W. Brent Edwards, Alan Hreljac, Glenn S. Fleisig, Kevin E. Wilk, Claude T. Moorman, Lonnie Paulos, and James R. Andrews. “Cruciate ligament tensile forces during the forward and side lunge.” Clinical Biomechanics 25.3 (2010): 213-21. Web.
- Fleming, Braden C., Heidi Oksendahl, and Bruce D. Beynnon. “Open- or Closed-Kinetic Chain Exercises After Anterior Cruciate Ligament Reconstruction?” Exercise and Sport Sciences Reviews 33.3 (2005): 134-40. Web.
- Heijne, Annette, Braden C. Fleming, Per A. Renstrom, Glenn D. Peura, Bruce D. Beynnon, and Suzanne Werner. “Strain on the Anterior Cruciate Ligament during Closed Kinetic Chain Exercises.” Medicine & Science in Sports & Exercise 36.6 (2004): 935-41. Web.
- Pandy, Marcus G., and Kevin B. Shelburne. “Dependence of cruciate-ligament loading on muscle forces and external load.” Journal of Biomechanics 30.10 (1997): 1015-024. Web.
- Lobb, R., Tumilty, S., & Claydon, L. S. (2012). A review of systematic reviews on anterior cruciate ligament reconstruction rehabilitation. Physical Therapy in Sport, 13(4), 270-278. doi:10.1016/j.ptsp.2012.05.001
- Stasi, S. D., Myer, G. D., & Hewett, T. E. (2013). Neuromuscular Training to Target Deficits Associated With Second Anterior Cruciate Ligament Injury. Journal of Orthopaedic & Sports Physical Therapy, 43(11). doi:10.2519/jospt.2013.4693
- 49. Louie, J., & Mote, C. (n.d.). Contribution of the Musculature to Rotatory Laxity and Torsional Stiffness at the Knee. Skiing Trauma and Safety: Sixth International Symposium. doi:10.1520/stp23173s
- Markolf, K., Mensch, J., & Amstutz, H. (1976). Stiffness and laxity of the knee–the contributions of the supporting structures. A quantitative in vitro study. The Journal of Bone & Joint Surgery, 58(5), 583-594. doi:10.2106/00004623-197658050-00001
- Solomonow, M., Baratta, R., Zhou, B., Shoji, H., Bose, W., Beck, C., & Dambrosia, R. (1987). The synergistic action of the anterior cruciate ligament and thigh muscles in maintaining joint stability. The American Journal of Sports Medicine, 15(3), 207-213. doi:10.1177/036354658701500302
- Paterno, M. V., Schmitt, L. C., Ford, K. R., Rauh, M. J., Myer, G. D., Huang, B., & Hewett, T. E. (2010). Biomechanical Measures During Landing and Postural Stability Predict Second Anterior Cruciate Ligament Injury After Anterior Cruciate Ligament Reconstruction and Return to Sport. The American Journal of Sports Medicine, 38(10), 1968-1978. doi:10.1177/0363546510376053
- Konishi, Y., Fukubayashi, T., & Takeshita, D. (2002). Possible mechanism of quadriceps strength relative to body weight: a risk factor for knee osteoarthritis in women? Med sci sports exerc, 34, 1414-1418.
- Koga, H., Nakamae, A., Shima, Y., Iwasa, J., Myklebust, G., Engebretsen, L., . . . Krosshaug, T. (2010). Mechanisms for Noncontact Anterior Cruciate Ligament Injuries: Knee Joint Kinematics in 10 Injury Situations From Female Team Handball and Basketball. The American Journal of Sports Medicine, 38(11), 2218-2225. doi:10.1177/0363546510373570
- Thomeé, R., Kaplan, Y., Kvist, J., Myklebust, G., Risberg, M. A., Theisen, D., . . . Witvrouw, E. (2011). Muscle strength and hop performance criteria prior to return to sports after ACL reconstruction. Knee Surgery, Sports Traumatology, Arthroscopy, 19(11), 1798-1805. doi:10.1007/s00167-011-1669-8
- Braitenberg, V., & Atwood, R. P. (1958). Morphological observations on the cerebellar cortex. The Journal of Comparative Neurology, 109(1), 1-33. doi:10.1002/cne.901090102
- Welsh, J. P., Lang, E. J., Suglhara, I., & Llinás, R. (1995). Dynamic organization of motor control within the olivocerebellar system. Nature, 374(6521), 453-457. doi:10.1038/374453a0
- Keele, S. W., & Ivry, R. (1990). Does the Cerebellum Provide a Common Computation for Diverse Tasks? A Timing Hypothesis. Annals of the New York Academy of Sciences, 608(1 The Development), 179-211. doi:10.1111/j.1749-6632.1990.tb48897.x
- Oreilly, J. X., Mesulam, M. M., & Nobre, A. C. (2008). The Cerebellum Predicts the Timing of Perceptual Events. Journal of Neuroscience, 28(9), 2252-2260. doi:10.1523/jneurosci.2742-07.2008
- Holmes, G. (1917). The Symptoms Of Acute Cerebellar Injuries Due To Gunshot Injuries. Brain, 40(4), 461-535. doi:10.1093/brain/40.4.461
- Diener, H., & Dichgans, J. (1992). Pathophysiology of cerebellar ataxia. Movement Disorders, 7(2), 95-109. doi:10.1002/mds.870070202
- Tanaka, M., Ishii, A., & Watanabe, Y. (2013). Neural Mechanism of Facilitation System during Physical Fatigue. PLoS ONE, 8(11). doi:10.1371/journal.pone.0080731
- Quatman, C. E., A. Kiapour, C. K. Demetropoulos, A. Kiapour, S. C. Wordeman, J. W. Levine, V. K. Goel, and T. E. Hewett. “Preferential Loading of the ACL Compared to the MCL during Landing: A Novel In Sim Approach Yields the Multi-Planar Mechanism of Dynamic Valgus during ACL Injury.” Orthopaedic Journal of Sports Medicine 1.4 Suppl (2013): n. pag. Web.
- Hosseini, A., Li, J., Gill, T. J., & Li, G. (2014). Meniscus Injuries Alter the Kinematics of Knees With Anterior Cruciate Ligament Deficiency. Orthopaedic Journal of Sports Medicine, 2(8), 232596711454734. doi:10.1177/2325967114547346
- Barker, T., Martins, T. B., Hill, H. R., Kjeldsberg, C. R., Trawick, R. H., Weaver, L. K., & Traber, M. G. (2011). Low Vitamin D Impairs Strength Recovery After Anterior Cruciate Ligament Surgery. Journal of Evidence-Based Complementary & Alternative Medicine, 16(3), 201-209. doi:10.1177/2156587211413768
- Dragoo, J. L., Castillo, T. N., Braun, H. J., Ridley, B. A., Kennedy, A. C., & Golish, S. R. (2011). Prospective Correlation Between Serum Relaxin Concentration and Anterior Cruciate Ligament Tears Among Elite Collegiate Female Athletes. The American Journal of Sports Medicine, 39(10), 2175-2180. doi:10.1177/0363546511413378
- Beckett, M. E., Massie, D. L., Bowers, K. D., & Stoll, D. A. (1992). Incidence of hyperpronation in the ACL-injuried knee: a clinical perspective. Journal of athletic training, 27, 58-62.
- Kramer, L. C., Denegar, C. R., & Buckley, W. E. (2007). Factors associated with anterior cruciate ligament injury history in female athletes. Journal of sports medicine and physical fitness, 47(4), 446-454.
- Barker T, Marins T, Hill H, Kjeldsberg C, Trawick R, Weaver L, Traber M. Low vitamin D impairs strength recovery after anterior cruciate ligament surgery. Journal of evidence-based complementary & alternative Medicine. 2011(16);3:201-209.
- Jenkins, W. L., Raedeke, S. G., & Williams, D. B. (2008). The Relationship Between the Use of Foot Orthoses and Knee Ligament Injury in Female Collegiate Basketball Players. Journal of the American Podiatric Medical Association, 98(3), 207-211. doi:10.7547/0980207
- Gong, W., Ro, H., Park, G., & Kim, T. (2011). The Influence of Pelvic Adjustment on Functional Leg Length Inequality and Foot Pressure. Journal of Physical Therapy Science, 23(1), 17-19. doi:10.1589/jpts.23.17
- Kibler, B., Press, J., & Sciascia, A. (2006). The Role of Core stability in the Athletic function. Sports medicine, 36(3), 189-198.