
The Truth about Concussions
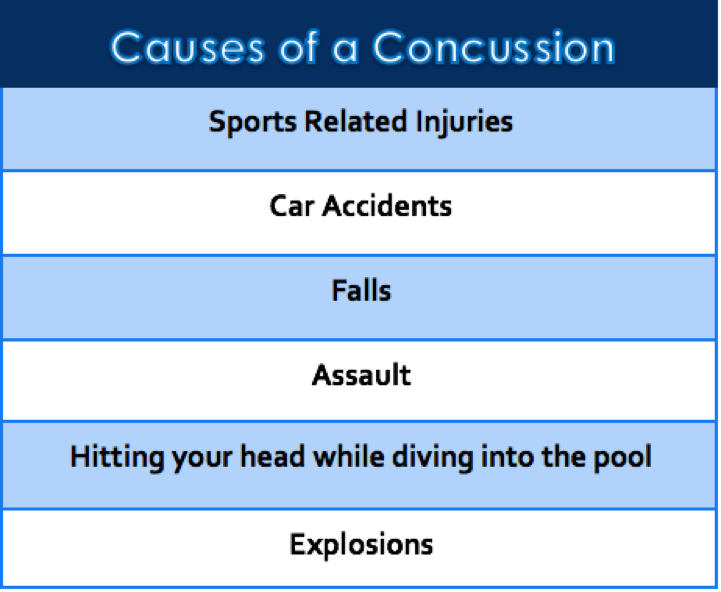
With kids back in school and football in season on the horizon, the topic of concussions may currently be a popular concern among players and parents. There will most likely be someone you know or know of that will experience a concussion this year. Your brain is your most valuable organ in your body because it controls and coordinates all other functions within your body. Concussions increased from 300,000 in 2001 to 4 million in 2011,1,2 however, as many as 50% of concussions go unreported.3 More than 1,000,000 mild traumatic brain injuries4 and an estimated 1.6-3.8 million sport-related concussions occur every year in the United states.5 This is a huge problem that needs to be addressed and taken more seriously.
What Is a Concussion?
Concussions have a historical meaning of a low velocity injury that causes the brain to get shaken within the skull. Concussions are more of a functional problem rather than structural one.6 A Concussion is a brain injury that has a pathophysiological effect on the brain, induced by biomechanical forces6 that juggle the brain around within the skull. In the past, damage from concussions and head injuries in the sports community were minimized and often overlooked to get players back on the field as soon as possible.7Concussions result in neuroinflammation in the brain that can persist after the initial injury.8 Now, we are seeing some of the long term effects and are starting to study them more to learn more about them.
Rotational forces are most damaging to the brain because they cause more damage to the neurons themselves.8,9–13These rotational forces cause shearing within the brain and is the primary mechanism of injury during a concussion.14-16 The same amount of force that it takes to cause a whiplash injury to the neck can cause a concussion, and they are very similar in terms of mechanism of injury and often occur at the same time.
Pathophysiology of a Concussion:
When a concussion occurs, the cellular membranes of neurons are damaged and excitatory neurotransmitters are released causing misfiring of nerves and ionic imbalances occur simultaneously. The high amount of force involved with a traumatic brain injury is sufficient to damage the microtubules in axons in the brain, causing them to rupture.17 This this significant because the break in the axons interferes with transport of materials in the cells, not allowing them to function efficiently. Since cells are damaged there is an increase in uptake of ATP (energy currency of a cell) to help repair the damaged cells and balance the ionic imbalances. This also means there is an increase in glucose by the brain within 24 hours after a concussion, but is sometimes hindered getting to the brain by a decrease in cerebral blood flow from the inflammation that occurs simultaneously from the concussion. 5,18-21 The process is know as the metabolic cascade.
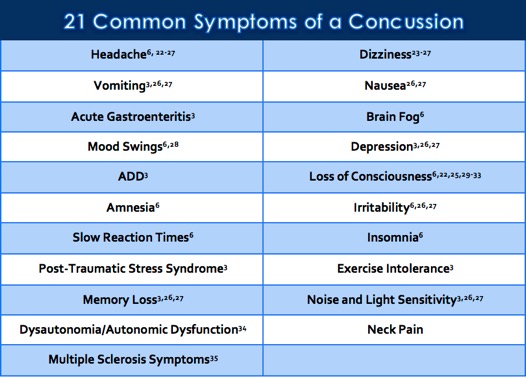
Loss of consciousness only occurs in 8-19% of concussions and is not a defining feature.30,36 For most people, symptoms typically resolve 80-90% within 7 days after a concussion.37,22-24,31 Unfortunately, headaches, dizziness38,39, fatigue,26,27 tiredness, fogginess24 at the time of the concussion are some symptoms that are usually associated with longer recovery times. If a concussion damages the hippocampus, amygdala, or prefrontal region of the brain, then that person may be prone to having emotional or mood problems since those areas of the brain can greatly influence them.3 Sometimes, migraines can be so bad after a concussion that light and noise can exacerbate the migraine, leaving one feeling uncomfortable and irritable. It is not uncommon for symptoms to get worse in the days following a concussion, especially with exercise or significant cognitive exertion.40 This suggests that even though someone may no longer have symptoms, their bodies may still have an underlying problem going undetected. The cervical spine can have involvement with headaches following a concussion41, especially the upper cervical spine.42,43 When the cervical spine is out of alignment it can also affect the function of the vestibular system which can play a role with dizziness and balance post concussion. A study done by Hurwitz et al found that the cervical spine was involved in all individuals who had a concussion.44 This suggests that people who have had a concussion should get their neck checked by a chiropractor to see if they have a subluxation. A chronic history of concussions increase your risk for developing neurodegenerative diseases, such as chronic traumatic encephalopathy (CTE) and dementia.45-48 In a 9 year study, retired professional football players that reported 3 or more concussions were 3 times more likely to be diagnosed with depression compared to athletes that reported no concussions.49 A study published in Nature Reviews Neurology found that a single diagnosis during the adolescence years increased your risk of developing MS by 22%, and individuals who have suffered two or more concussions increased their risk of MS by 133%!35
Diagnosis:
There is currently no gold standard test for diagnosing concussions.50 It is challenging to determine if any neurons in one’s brain have been damaged with the technology we have today, other than dissection after someone has ceased.6,51 The majority of patients with a mild traumatic brain injury will have a normal Glasgow coma scale of 15, which means we need to find other ways to quantify the damage that is being done when a concussion occurs, not just rely on the symptoms. The majority of sport related concussions do not require neuroimaging.52-57 Since a concussion represents more of a functional problem than a structural one, CT scans and MRIs are almost always negative.6,58-64 Only 5-8% of traumatic brain injury patients will have a CT-positive scan,65 but are necessary to detect skull fractures, swelling of the brain, intracranial hemorrhage, and any other anatomical pathologies that might be present or life threatening.6 Most of the time, the results are negative because there is no way to see axonal damage in the brain with imaging at this point in time.6,58-64 Hopefully, new technology will be developed in the future so we will be able to see the damage and quantify it. Athletic trainers and primary sports physicians are great at detecting these life threatening traumas. The scary part is the effects of concussions are cumulative over time66,67, especially if one has not recovered from a current concussion.19,21,68-72 This means that even if you feel fine after a concussion in the past, the damage accumulates in the brain over time if recurrent concussions are happening. Even subconcussive blows to the head can be cumulative73,74 and pathological to the brain.3,75
Only your medical doctor can determine if medication is necessary, but keep in mind that taking pharmaceuticals can mask the symptoms of a concussion. This is a great concern because if we are determining if someone has gotten better after a concussion based how they feel while taking medications, the results can be misleading.6 In some cases, it is best to avoid anti-inflammatory pain medication in order to minimize bleeding risk and cover up symptoms the concussion may be producing.40
What Type of Helmets Are Best?

Currently, there is a great market for helmets that may be able to reduce the risk of concussion. Helmets provide protection to the head by absorbing impacting forces and diffusing them over a greater surface area.76 With the recent awareness of concussions over the past decade, there have been many people trying to design special helmets to help to prevent concussions or marketing helmets with such claims. Making sure the helmet fits properly is most important so the helmet has less room to float around and possibly slide off. As of right now, there is insufficient data to support one type of football helmet over others when it comes to preventing concussions.25,77,78 However, no matter how good the helmet is, it is the abrupt outside forces that cause the brain to get shaken within the skull itself. There is no helmet that can prevent the brain from getting shaken within the skull under contact sports! Most people think just because you have a helmet on that your head is protected. This is true to some extent, because your skull is more protected from getting lacerations, fractures and bruised, but this does not prevent the brain from getting shaken within the skull and reduce your risk of concussion.25,79-82
Should you Exercise after a Concussion?

There is great debate over whether someone should exercise post concussion. Some questions that arise when this topic is brought up are; how long after a concussion should someone start to exercise? What type of intensity? What type of exercise? Does the degree of the concussion play a factor? Low-level exercise for those who are slow to recover may be beneficial, but this can vary person to person.6 One study done by Majerke et al found that performing high levels of activity after a concussion worsened neurocognitive performance.83 Physical exercise was found to have a statistically significant improvement in the post-concussion symptom scale score and symptoms in patients with a concussion.84 Monitoring your progress and trying not to push yourself during the acute stage after a concussion is important. You are the best predictor of how you are doing, so if you feel yourself getting worse then you should cut your exercises back and gradually build up.
How to Minimize Risk?
- Playing a sport, like soccer, that requires you to head the ball, it helps to properly tense the muscles of the back and neck in preparation to head the ball.7
- Neck strengthening exercises to increase stability of the cervical spine for better control of the head105,106
- Limit the number of contact practices to reduce exposures to potential concussions3
- Reducing illegal tackles such as high tackles in Rugby can reduce risk
How Can Chiropractic Help with Concussions?
When many people get a concussion, they often don’t think of going to a chiropractor for help during the recovery process. The brain is the most important organ in the body and the brain stem extends down to the first and second vertebrae in your neck. If these bones become misaligned during the whiplash/concussion, they can affect the function of the brain.
The brain needs 3 things to function:
- Oxygen
- Energy (glucose/ketones)
- Stimulation
Oxygen is important for the metabolic process in our cells (oxidative phosphorylation). If our spine is subluxated, affecting the nerves going to the lungs, it can decrease the function of our lungs. From a more biomechanical point of view, if our rib cage cannot move properly, then our lungs won’t be able to expand as full as they should, decreasing the amount of possible oxygen that could be getting to our cells.107 It is important to get plenty of oxygen to meet the demands of our brain.

Adjustments can increase:
1. Oxygen intake108
2. Cerebrospinal fluid flow109
3. Neurological stimulation to the brain
4. Balance to the autonomic nervous system
Often times, the upper cervical spine can get misaligned putting tension on the suboccipital muscles, especially rectus capitis posterior minor. This is directly attached to the dura matter110, which may play a role in recovery and symptomatology a person may experience after a concussion.111 The dura is also innervated by the first 3 cervical nerves, which converge with the trigeminal nerve in the trigeminal nucleus. Rotation in C1 and C2, disc herniations C4-C7, and chiari malformations have been found to decrease cerebral spinal fluid flow totally and partially to the brain found using UPRIGHTⓇ CSF flow by the FONAR UPRIGHTⓇ Multi-PositionTM MRI. This is a special type of MRI that is used to see cerebrospinal fluid moving in real time. This is huge in the research world! Decreased CSF could be a contributing factor in the recovery process after a concussion and should definitely be considered.109 Spinal adjustments can help to align the spine, improving CSF flow, making nutrients more available to the brain and spinal cord.
If there is lack of motion in the spine, then it will send less sensorimotor input into the brain. Adjustments given to areas of the spine that are not moving properly can increase neurological input, stimulating areas of the brain, giving the brain a boost.
Misalignments in the spine can cause an imbalance in the autonomic nervous system decreasing vagal tone (rest and digest mode), which is important during the healing process and overall health especially when dealing with a concussion. If the spine becomes misaligned affecting the vagus nerve or vagal tone of the body then many digestive and other health related problems can arise as a result.
How a Concussion Can Affect My Performance?
After a collegiate football player sustains a concussion, they are 2.5 times more likely to sustain a lower extremity injury or ligamentous injury than uninjured teammates.112-114 This is thought to be because of unresolved neuromuscular impairments. I would suggest that there are interferences within the nervous system coming from subluxations in the spine, or damage in specific areas of the brain, leading to neuromuscular deficits. With a decrease in neuromuscular control as a result, this means the ligamentous structures in the knees and ankles will be more stressed and be more likely to get injured as a result.115 A decrease in voluntary contraction has been demonstrated in ice hockey players116 and decrease in quadriceps strength has been demonstrated in college football players after a concussion.117 All skeletal muscles are under neurological control. If the nervous system cannot communicate properly with the muscles, then you have a loss of neuromuscular control. Adjustments can help to improve the neuromuscular control, by removing neurological interference that may be caused by subluxations in the spine.

The damaging effects from concussions have received more attention the past decade due to social media and athletes speaking out about it. Even if you do not have symptoms from a concussion, it does not mean no damage has been done and symptoms can vary from person to person. Right now, there is no definitive objective test that can be used to verify if you have had a concussion. There is no helmet on the market that can prevent a concussion from occurring, you can only minimize your risk while playing sports or extracurricular activities. Chiropractic focuses on restoring the brain and nervous system back to normal and can be a great way to help recover from a concussion!
Resources
- Broglio SP, Eckner JT, Martini D, Sosnoff JJ, Kutcher JS, Randolph C. Cumulative head impact burden in high school football. J Neurotrauma. 2011;28:2069-2078
- Covassin T, Swanik CB, Sachs ML. Epidemiological considerations of concussions among intercollegiate athletes. Appl Neuropsychol. 2003;10:12-22.
- Harmon K, Drezner J, Gammons M, et al. American medical society for sports medicine position statement: concussion in sport. Clin J Sport Med. 2013;23:1-18.
- Bazarian JJ, McClung J, Shah MN, Cheng YT, et al. Mild traumatic brain injury in the United States, 1998-2000. Brain Inj. 2005;19(2):85-91.
- Ellis M.J., Leddy J.J., Willer B. Physiological, vestibule-ocular and cervicogenic post-concussion disorders: An evidence-based classification system with directions for treatment. Brain Inj. 2014;29:238-248.
- McCrory P, Meeuwisse W, Aubry M, et al. Consensus statement on concussion in sport: the 4th international conference on concussion in sport held in Zurich, November 2012
- Barth J, Freeman J, Broshek D, Varney R. Acceleration-Deceleration sport-related concussion: The gravity of it all. Journal of Athletic Training. 2001;36(3):253-256.
- Rathbone AT, Tharmaradinam S, Jiang S, et al. A review of the neuro- and systemic inflammatory responses in post concussion symptoms: Introduction of the “post-inflammatory brain syndrome” PIBS. Brain Behav Immun 2015;46:1-16. Doi: 10.1016/j.bbi.2015.02.009
- Takhounts EG, Crandall JR, Darvish K. On the importance of nonlinearity of brain tissue under large deformations. Stapp Car Crash J. 2003; 47:79–92. [PubMed: 17096245]
- Miller K, Chinzei K. Constitutive modelling of brain tissue: experiment and theory. J Biomech. 1997; 30(11–12):1115–21. [PubMed: 9456379]
- Donnelly BR, Medige J. Shear properties of human brain tissue. J Biomech Eng. 1997; 119(4): 423–32. [PubMed: 9407281]
- Arbogast KB, Thibault KL, Pinheiro BS, et al. A high-frequency shear device for testing soft biological tissues. J Biomech. 1997; 30(7):757–9. [PubMed: 9239559]
- Prange MT, Meaney DF, Margulies SS. Defining brain mechanical properties: effects of region, direction, and species. Stapp Car Crash J. 2000; 44:205–13. [PubMed: 17458728]
- Unterharnscheidt F, Higgins LS. Traumatic lesions of brain and spinal cord due to non-deforming angular acceleration of the head. Tex Rep Biol Med. 1969; 27(1):127–66. [PubMed: 4976573]
- Gennarelli TA, Thibault LE, Adams JH, et al. Diffuse axonal injury and traumatic coma in the primate. Ann Neurol. 1982; 12(6):564–74. [PubMed: 7159060]
- Adams JH, Graham DI, Murray LS, et al. Diffuse axonal injury due to non-missile head injury in humans: an analysis of 45 cases. Ann Neurol. 1982; 12(6):557–63. [PubMed: 7159059]
- Ahmadzadeh H, Smith D, Shenoy V. Mechanical effects of dynamic binding between tau proteins on microtubules during axonal injury. Biophysical J. 2015;2328-2337
- Giza CC, Hovda DA, The neurometabolic cascade of concussion. J Athl Train. 2001;36(3):228-235.
- Prins ML, Hales A, Reger M, et al. Repeat traumatic brain injury in juvenile rat is associated with increased axonal injury and cognitive impairments. Dev Neurosci. 2010;32:510-518.
- Barkhoudarian G, Hovada DA, Giza CC. The molecular pathophysiology of concussive brain injury. Clin Sports Med. 2011;30:33-48
- Vagnozzi R, Tavazzi B, Signoretti S, et al. Temporal window of metabolic brain vulnerability to concussions: mitochondrial-related impairment Part I. Neurosurgery. 2007;61:379-388.
- Meehan WP III, d’Hemecourt P, Comstock RD. High school concussions in the 2008-2009 academic year: mechanism, symptoms, and management. Am J Sports Med. 2010;38:2405-2409.
- Marar M, McIlvain NM, Fields SK, et al. Epidemiology of concussions among United States high school athletes in 20 sports. Am J Sports Med. 2012;40:747-755.
- Makdissi M, Darby D, Maruff P, et al. Natural history of concussion in sport: markers of severity and implications for management. Am J Sports Med. 2010;38:464-471.
- Benson BW, Hamilton GM, Meeuwisse WH, et al. Is protective equipment useful in preventing concussion? A systematic review of the literature. Br J sports Med. 2009;43:56-67
- Kushner D, Mild traumatic brain injury: Toward understanding manifestations and treatment. Arch. Inter. Med. 1998;158:1617
- Alexander MP, Mild traumatic brain injury: Pathophysiology, natural history, and clinical management. Neurology. 1995;45:1253-1260
- Busch CR, Alpern HP. Depression after mild traumatic brain injury: a review of current research. Neuropsychol Rev 1998;8:95–108.
- McCrory P, Meeuwisse W, Johnston K, et al. consensus statement on concussion in sport, 3rd International Conference on Concussion in sport held in Zurich, November 2008. Br J Sports Med. 2009;43:76-90
- Collins MW, Iverson GL, Lovell MR, et al. On-field predictors of neurophysiological and symptom deficit following sports-related concussion. Clin J Sport Med. 2003;13:222-229
- McCrea M, Barr WB, Guskiewicz K, et al. Standard regression-based methods for measuring recovery after sport-related concussion. J Int Neuropsychol Soc. 2005;11:58-69
- McCrory P. Refshauge lecture. When to retire after concussion? J sci Med sport. 2002;5:169-182
- Mansell JL, Tierney RT, Higgins M, et al. Concussive signs and symptoms following head impacts in collegiate athletes. Brain Inj. 2010;24:1070-1074.
- Esterov D, Greenwald B. Autonomic Dysfunction after mild traumatic brain injury. Brain sci. 2017;11:1-8
- Montgomery S, et al. Concussion in adolescence and risk of multiple sclerosis. Ann Neurol. http://dx.doi.org/10.1002/ana.25036
- Shulz MR, Marshall SW, Mueller FO, et al. Incidence and risk factors for concussion in high school athletes, North Carolina, 1996-1999. Am J Epidemiol. 2004;160:937-944
- McCrea M, Guskiewicz KM, Marshall SW, et al. Acute effects and recovery time following concussion in collegiate football players: the NCAA concussion study. JAMA. 2003;290(19):2556-2563.
- Lau B, Lovell MR, Collins MW, et al. Neurocognitive and symptom predictors of recovery in high school athletes. Clin J Sport Med 2009;19:216–21.
- Lau BC, Kontos AP, Collins MW, et al. Which on-field signs/symptoms predict protracted recovery from sport-related concussion among high school football players? Am J Sports Med 2011;39:2311–18.
- Kutcher J MD, Giza C MD. Sports concussion diagnosis and management. Continuum Journal.2014;1563.
- Treleaven J, Jull G, Atkinson L. Cervical musculoskeletal dysfunction in post-concussional headache. Cephalalgia. 1994;14:273-9
- Bogduk N. The neck and headaches. Neurol Clin N Am. 2004;22:151-71
- Hecht J. Occipital nerve blocks in postconcussive headaches: a retrospective review and report of ten patients. J Head Trauma Rehabil. 2004;19:58-71.
- Hurwitz E, Carragee EJ, van der Velde G, et al. Treatment of neck pain: noninvasive interventions: results of the bone and joint decade 2000-2010 task force on neck pain and its associated disorders. Spine. 2008;15:s123-52
- Delaney JS, Lacroix VJ, Gagne C, Antioniou J. Concussions among university football and soccer players: a pilot study. Clin J Sport Med. 2001;11:234-240.
- Iverson GL, Gardner AJ, McCrory P, Zafonte R, Castellani RJ. A critical review of chronic traumatic encephalopathy. Neurosci Biobehav Rev. 2015;56:276-293.
- Petraglia AL, Dashnaw ML, Turner RC, Bailes JE. Models of mild traumatic brain injury. Translation of physiological and anatomic injury. Neurosurgery 75 (suppl 4). 2014:S34-S49.
- Trotter BB, Robinson ME, Milberg WP, McGlinchey RE, Salat DH. Military blast exposure, ageing and white matter integrity. Brain. 2015;138:2278-2292.
- Kerr Z, Marshall S, Harding H, Guskiewicz K. Nine-year risk of depression diagnosis increases with increasing self-reported concussions in retired professional football players. Am J Sports Med. 2012;40:2206-2212.
- Broglio SP, Ferrara MS, Macciocchi SN, Baumgartner TA, Elliott R. Test-retest reliability of computerized concussion assessment programs. J Athl train. 2007;42:509-514.
- Breedlove E, Robinson M, Talavage T, et al. Biomechanical correlates of symptomatic and asymptomatic neurophysiological impairment in high school football. J Biomechanics. 2012;45:1265-1272.
- Davis GA, Iverson GL, Guskiewicz KM, et al. Contributions of neuroimaging,balance testing, electrophysiology and blood markers to the assessment of 179 sport-related concussion. Br J Sports Med 2009;43(Suppl 1):i36–45.
- Smits M, Houston GC, Dippel DW, et al. Microstructural brain injury in post-concussion syndrome after minor head injury. Neuroradiology 180 2011;53:553–63.
- Pulsipher DT, Campbell RA, Thoma R, et al. A critical review of neuroimaging applications in sports concussion. Curr Sports Med Rep 2011;10:14–20. 181
- Prabhu SP. The role of neuroimaging in sport-related concussion. Clin Sports Med 2011;30:103–14, ix.
- Echemendia RJ, Putukian M, Mackin RS, et al. Neuropsychological test 182 performance prior to and following sports-related mild traumatic brain injury. Clin J Sport Med 2001;11:23–31.
- Amen DG, Trujillo M, Newberg A, et al. Brain spect imaging in complex psychiatric cases: an evidence-based, underutilized tool. Open Neuroimag J. 2011;5:40–8.
- Giza C, Kutcher J, Ashwal S, et al. Summary of evidence-based guideline update: Evaluation and management of concussion in sports: Report of the guideline development subcommittee of the American academy of neurology. American Academy of Neurology. 2013
- Broglio SP, Cantu RC, Gioia GA, et al. National Athletic Trainers’ Association position statement: management of sport concussion. J Athl Train. 2014;49:245-265.
- Halstead ME, Walter KD. American Academy of Pediatrics. Clinical report-sport-related concussion in children and adolescents. Pediatrics. 2010;126:597-615.
- Harmon KG, Drezner J, Gammons M, et al. American Medical Society for Sports Medicine position statement: concussion in sport. Clin J Sport Med. 2013;23:1-18.
- Barr WB. Mild traumatic brain injury, in sherer M, Sander AM (eds). Handbook neuropsychology of traumatic brain injury. New York. 2014;347-369.
- Blennow K, Hardy J, Zetterberg H. The neuropathology and neurobiology of traumatic brain injury. Neuron. 2012;76:886-899.
- Corso P, Finkelstein E, Miller T, Fiebelkorn I, Zaloshnja E. Incidence and lifetime costs of injuries in the United States. Inj Prev. 2006;12:212-22
- Lagerstedt L, Egea-Guerrero J, Bustamante A, et al. H-FABP: A new biomarker to differentiate between CT-positive and CT-negative patients with mild traumatic brain injury. PLos One. 2017;12(4):1-11
- Collins, M, Lovell M, Iverson G, et al. Cumulative effects of concussion in high school athletes. Neurosurgery. 2002;5:1175-1179
- Guskiewicz K, McCrea M, Marshall S, et al. Cumulative effects associated with recurrent concussion in collegiate football players: the NCAA concussion study. JAMA. 2003;290(19):2549-2555
- Shrey DW, Griesbach GS, Giza CC. The pathophysiology of concussions in your. Phys Med Rehabil Clin N Am. 2011;22:577-602
- Vagonzzi R Signoretti S, Tavazzi B, et al. Temporal window of metabolic brain vulnerability to concussion: a pilot 1h-magnetic resonance spectroscopic study in concussed athletes Part III. Neurosurgery. 2008;62:1286-1295
- Tavazzi B, Vagnozzi R, Signoretti S, et al. Temporal window of metabolic brain vulnerability to concussion: oxidative and nitrosative stresses Part II. Neurosurgery. 2007;61:390-395
- Esposito G, Van Horn JD, Weinberger Dr, et al. Gender differences in cerebral blood flow as a function of cognitive state with pet. J Nucl Med. 1996;37:559-564
- Longhi L, Saatman KE, Fujimoto S, et al. Temporal window of vulnerability to repetitive experimental concussive brain injury. Neurosurgery. 2005;56:364-374
- Field Hearing: legal issues relating to football head injuries. Part II written statement by bennet. Omalu, MD, MBA, MPH. Committee on the Judiciary. 2010.
- McKee A, Cantu R, Nowinski C, et al. Chronic traumatic encephalopathy in athletes: progressive tauopathy after repetitive head injury. J. Neuropathol. Exp. Neurol. 2009;68(7):709-735.
- Talavage T, Nauman E, Breedlove E, et al. Functionally-detected cognitive impairment in high school football players without clinically-diagnosed concussion. J Neurotrauma. 2010. Submitted Manuscript.
- Medina M, Avila J. New perspectives on the role of tau in Alzheimer’s disease. Implications for therapy. Biochem Pharmacol. 2014;88:540-547.
- Giza CC, Kutcher JS, Ashwal S, et al. Summary of evidence-based guideline update: evaluation and management of concussion in sports: report of the Guideline Development Subcommittee of the American Academy of Neurology. 2013;80:2250-2257.
- Thompson DC, Rivara FP, Thompson R: Helmets for preventing head and facial injuries in bicyclists. Cochrane Database Syst Rev. 2000;2.
- Daneshvar DH, Baugh CM, Nowinski CJ, et al. Helmets and mouth guards: the role of personal equipment in preventing sport-related concussions. Clin Sports Med 2011;30:145–63, x.
- Navarro RR. Protective equipment and the prevention of concussion—what is the evidence? Curr Sports Med Rep 2011;10:27–31.
- McCrory P. Sport concussion assessment tool 2. Scand J Med Sci Sports 126. 2009;19:452.
- McCrory P. Do mouthguards prevent concussion? Br J Sports Med 2001;35:81–2.
- Majerske C, Mihalik J, Ren D, et al. Concussion in sports: postconcussive activity levels, symptoms, and neurocognitive performance. J Athletic training. 2008;43(3):265-274.
- Lal A, Kolakowsky-Hayner S.A, Ghajar J, Balamane M. The effect of physical exercise after a concussion: A systematic review and meta-analysis. Am J Sports Med. 2017.
- Abrahams S, Fie S, Patricios J, Posthumus M, et al. Risk factors for sports concussion: an evidence-based systematic review. Br J Sports Med. 2014;48:91-97
- Schulz MR, Marshall SW, Mueller FO, et al. Incidence and risk factors for concussion in high school athletes, North Carolina, 1996-1999. Am J Epidemiol. 2004;160:937-944.
- Colvin AC, Mullen J, Lovell MR, et al. The role of concussion history and gender in recovery from soccer-related concussion. Am J Sports Med. 2009;37:1699-1704.
- Emery C, Kang J, Shrier I, et al. Risk of injury associated with bodychecking experience among youth hockey players. CMAJ 2011;183:1249–56.
- Guskiewicz KM, Marshall SW, Bailes J, et al. Recurrent concussion and risk of depression in retired professional football players. Med Sci Sports Exerc 2007;39:903–9.
- Guskiewicz KM, McCrea M, Marshall SW, et al. Cumulative effects associated with recurrent concussion in collegiate football players: the ncaa concussion study. JAMA 2003;290:2549–55.
- Guskiewicz KM, Weaver NL, Padua DA, et al. Jr. Epidemiology of concussion in collegiate and high school football players. Am J Sports Med 2000;28: 643–50.
- Hollis SJ, Stevenson MR, McIntosh AS, et al. Incidence, risk, and protective factors of mild traumatic brain injury in a cohort of Australian nonprofessional male rugby players. Am J Sports Med 2009;37:2328–33.
- Kristman VL, Tator CH, Kreiger N, et al. Does the apolipoprotein epsilon 4 allele predispose varsity athletes to concussion? A prospective cohort study. Clin J Sport Med 2008;18:322–8.
- Gessel LM, Fields SK, Collins CL, et al. Concussions among United States high school and collegiate athletes. J Athletic Training 2007;42:495–503.
- Lincoln AE, Caswell SV, Almquist JL, et al. Trends in concussion incidence in high school sports: a prospective 11-year study. Am J Sports Med 2011;39:958–63.
- Covassin T, Swanik CB, Sachs ML. Sex differences and the incidence of concussions among collegiate athletes. J Athletic Training 2003;38:238–44.
- Dick RW. Is there a gender difference in concussion incidence and outcomes? Br J Sports Med 2009;43(Suppl 1):i46–50.
- Pellman EJ, Powell JW, Viano DC, et al. Concussion in professional football: epidemiological features of game injuries and review of the literature—part 3. Neurosurgery 2004;54:81–94; discussion 86–94
- Giza CC, Hovda DA. The neurometabolic cascade of concussion. J Athletic Training 2001;36:228–35.
- Zuckerman SL, Odom M, Lee YM, et al. 145 sport-related concussion and age: number of days to neurocognitive baseline. Neurosurgery 2012;71:E558.
- Field M, Collins MW, Lovell MR, et al. Does age play a role in recovery from sports-related concussion? A comparison of high school and collegiate athletes. J Pediatr 2003;142:546–53.
- Moser RS, Schatz P, Jordan BD. Prolonged effects of concussion in high school athletes. Neurosurgery 2005;57:300–6; discussion.
- Sim A, Terryberry-Spohr L, Wilson KR. Prolonged recovery of memory functioning after mild traumatic brain injury in adolescent athletes. J Neurosurg 2008;108:511–16.
- Davis G, Purcell L. The evaluation and management of acute concussion differs in young children. Br J Sports Med. 2014;48:98-101.
- Reid SE, Raviv G, Reid SE Jr. Neck muscle resistance to head impact. Aviat Space Environ Med 1981;52:78-84.
- Tierney RT, Sitler MR, Swanik CB, et al. Gender differences in head-neck segment dynamic stabilization during head acceleration. Sci Sports Exerc 2005;37:272-79.
- Moore K, Dalley II A, Agur A. Clinically oriented Anatomy. 6th ed. Philadelphia, PA: Lippincott Williams & Wilkins: 2010.
- Fedorchuk C, Lightsone D, Vukovic D. Improvements in lung function, dysautonomia and grip strength in a patient with multiple sclerosis following correction of vertebral subluxation using chiropractic BioPhysicsⓇ: A case study and selective review of literature. 2016;3:73-83
- http://www.fonar.com/news/032813.htm
- Gray H, Williams PL, Bannister LH. Gray’s Anatomy: The anatomical basis of Medicine and surgery. 38th ed. New York: Churchill Livingston; 1995:806.
- Fakhran S, Qu C, Alhilali L.M. Effect of the suboccipital musculature on symptom severity and recovery after mild traumatic brain injury. Spine. 2016;1556-1560.
- Brooks MA, Peterson K, Biese K, Sanfilippo J, Heiderscheit BC, Bell DR. Concussion increases odds of sustaining a lower extremity musculoskeletal injury after return to play among collegiate athletes. Am J Sports Med. 2016;19:0363546515622387
- Lynall RC, Mauntel TC, Padua DA, Mihalik JP. Acute lower extremity injury rates increase after concussion in college athletes. Med Sci Sports Exerc. 2015;47(12):2487-92.
- Nordstrom A, Nordstrom P, Edstrand J. Sports-related concussion increases the risk of subsequent injury by about 50% in elite male football players. Br J Sports Med. 2014;48(19):1447-50.
- Benjaminse A, Habu A, Sell TC, et al. Fatigue alters lower extremity kinematics during a single-leg stop-jump task. Knee Surg Sports Traumatol Arthrosc. 2007;16(4):400-7
- Ford KR, Myer GD, Hewett TE. Longitudinal effects of maturation on lower extremity joint stiffness in adolescent athletes. Am J Sports Med. 2010;38(9):1829-37
- Reed N, Taha T, Keightley ML. Concussion and strength performance in youth ice hockey players. Br J Sports Med. 2013;47(5):e1.
- Senthinathan A, Mainwaring L.M., Hutchison M. Heart rate variability of athletes across concussion recovery milestones: A preliminary study. Clin J. Sport Med. 2017;27:288-295.
- Thurman DJ, Branche CM, Sniezek JE. The epidemiology of sports related traumatic brain injuries in the United States: recent developments. J Head Trauma Rehabil. 1998;13(2):1-8.
- Vagonzzi R, Signoretti S, Cristofori L, et al. Assessment of metabolic brain damage and recovery following mild traumatic brain injury: a multicentre, proton magnetic resonance spectroscopic study in concussed patients. Brain. 2010;133:3232-3242.
- Frommer LJ, Gurka KK, Cross KM, et al. Sex differences in concussion symptoms of high school athletes. J Athl Train. 2011;46:76-84.
- Sone JY, Kondziolka D, Huang J, Samadani U. Helmet efficacy against concussion and traumatic brain injury: a review. J Neurosurg. 2016:1-14.